


I sat in a room full of hospital executives once. They were talking about “physician productivity metrics” and “workforce optimization.” I was the only person at the table who had operated on a patient that morning.
At some point, someone said the quiet part out loud: “The physicians are our highest-value assets.”
Assets. Not partners. Not professionals entrusted with lives. Assets.
I said, “Then why are you treating them like liabilities?” The room got very quiet.
That was several years ago. I thought it would get better. It hasn’t. The data now confirms what I’ve been watching happen from inside the OR.
The Numbers Are Worse Than You Think
The Physicians Advocacy Institute released its 2026 report in partnership with Avalere Health. I read the whole thing. Here is what it says:
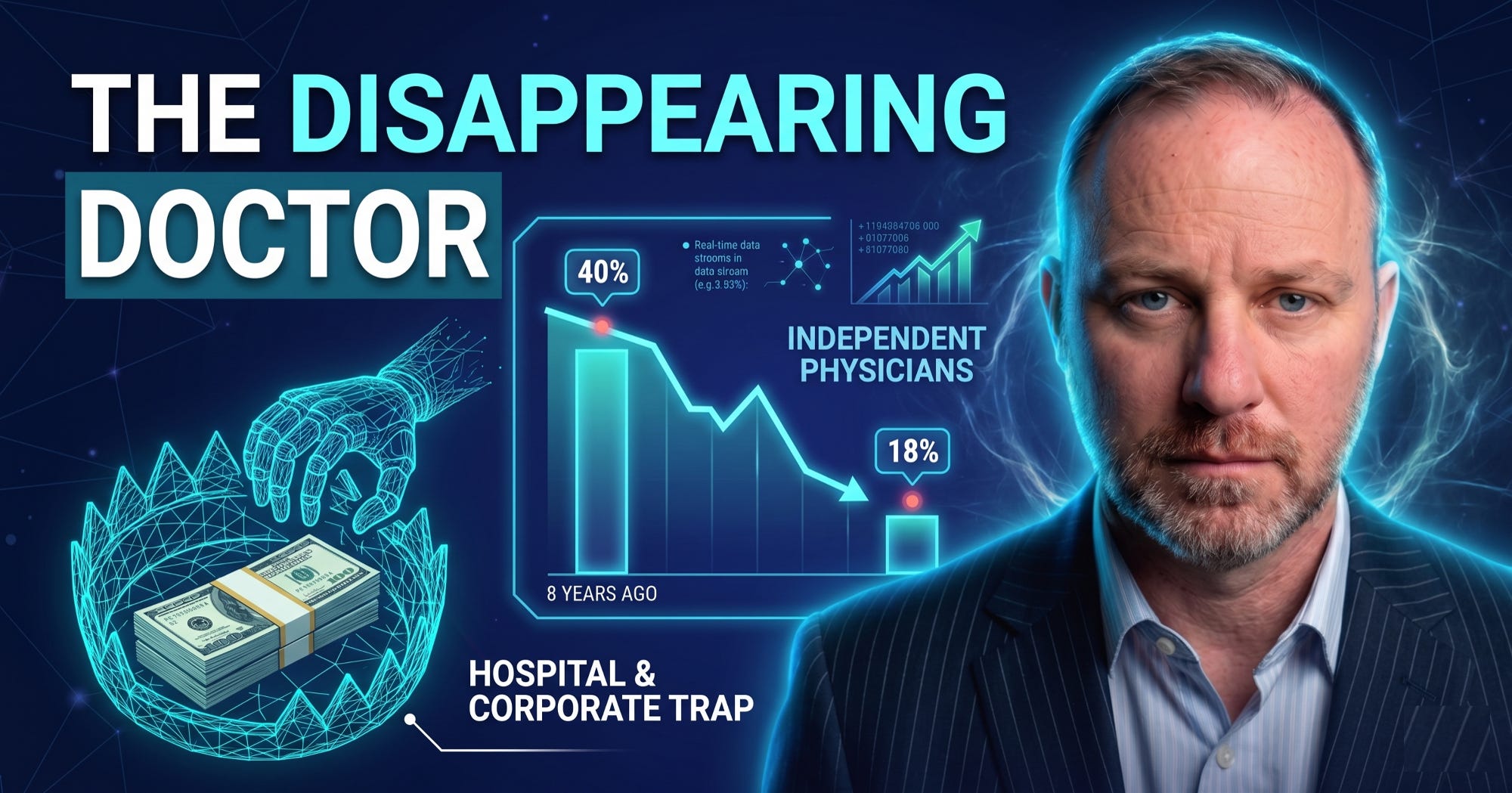
As of January 1, 2026, more than four in five physicians (82%) are now employed by hospitals or other corporate entities. More than six in ten physician practices (63.9%) are now owned by hospitals or other corporate entities.
Let that land.
Eight years ago, independent practice was the norm. Today it is the exception. Since 2018, 253,000 additional physicians became employees of hospitals or corporate entities. In that same period, 152,200 fewer physicians were operating independently.
This is not a slow drift. This is a controlled demolition.
The percentage of employed physicians grew by 5.6% from 2024 to 2026 alone, largely driven by hospital acquisition. The acceleration is not slowing. It is compounding.
And this isn’t a coastal or urban phenomenon. In rural areas, 80.2% of physicians are now employed and 67.8% of practices are now corporate or hospital owned, mirroring the national trend. The communities with the fewest healthcare options are the ones watching their local physicians get absorbed the fastest.
What “Employment” Actually Means
I want to be precise here, because the word “employment” sounds benign. It isn’t.
When a hospital system acquires a physician practice, several things happen. They don’t all show up in the press release.
First, clinical decision-making shifts. It doesn’t disappear overnight. It erodes over time, through scheduling pressures, through productivity quotas measured in relative value units, through prior authorization workflows that were designed not to protect patients but to delay or deny care. I’ve seen excellent surgeons spend 30 minutes on the phone fighting for a procedure they know their patient needs. That fight is with an administrator who has never been in an OR. And the surgeon loses more often than they should.
Second, the referral ecosystem locks in. Hospital systems don’t just hire physicians. They structure care delivery so that employed physicians refer within the system. That protects market share. It does not always protect the patient. I’ve had patients come to me after spending years inside a hospital system’s loop, never getting the surgical consultation they needed, because it was easier to keep billing for conservative management than to send them out.
Third, the financial architecture changes in ways that cost patients more. Corporate entity ownership of physician practices (33.2%) now outpaces hospital ownership (30.6%), and that matters because corporate owners, including private equity firms and health insurers, are optimizing for a return on investment, not a return to health. When a private equity group acquires a physician practice, the clock starts immediately. They are not there for the long game. They are there for the exit.

The Production Unit Problem
Here is what I know from building Indiana Orthopedic Institute from the ground up.
When we started, it was two people. We now have over 100 employees and 16 surgeons. We built it on a specific premise: that the physician should lead the organization, set the clinical standard, and bear direct accountability for outcomes. Not a committee. Not an administrator with a business degree and no clinical training. The surgeon.
That model is increasingly rare. And its rarity is not an accident.
The hospital and corporate acquisition model doesn’t fail because the people running it are malicious. It fails because the incentives are structurally misaligned. When a physician is an employee, their clinical judgment competes with their employment security. That is not a character flaw. It is a rational response to a bad system.
I have watched good surgeons stop pushing back. Not because they stopped caring about their patients. Because they got tired of fighting and losing. Because the system ground them down.
The PAI report puts a number on it. What it can’t quantify is the cumulative effect on patient care when the most experienced, most capable physicians in a system learn that dissent has consequences.
The “Security” Trap
The employment offer sounds attractive. Especially early in a career.
Guaranteed salary. Benefits. No overhead. No billing headaches. No administrative burden. Sign here, show up, operate, go home.
What the contract doesn’t spell out: You are transferring the most important professional asset you have. Not your license. Your autonomy.
I’m not arguing that employment is always wrong. Some physicians find genuine satisfaction in that structure, and there are employed settings where clinical independence is real. But those settings are increasingly the exception within large systems, not the rule.
What I am arguing is that most physicians sign those contracts without fully internalizing what they’re giving up, because the system doesn’t tell them. It is in the hospital’s interest for you not to think too hard about that. They need your clinical productivity. They do not need your clinical authority.
I said this to a group of residents a few years ago and one of them pushed back. “But what’s the alternative? Building something from scratch is terrifying.”
I said, “I know. I did it. It is terrifying. The question is whether you’re more afraid of that than you are of spending 30 years as someone else’s production unit.”
He went independent. He’s building something now.
The ASC Model Is the Most Important Structural Answer Nobody Talks About Enough
I want to be specific about what the alternative looks like, because vague calls for “physician autonomy” don’t build anything.
Ambulatory surgery centers are the most underutilized structural tool available to physicians who want to reclaim ownership of their practice environment.
The data on ASCs is not ambiguous. Costs are lower. Outcomes are comparable or better for the procedures they’re designed to handle. Patient satisfaction scores consistently outperform hospital outpatient departments. And the physician is not just a provider in that setting. The physician is an owner.
CMS has been slowly expanding the approved procedure list for ASCs, which means the scope of what can be done outside the hospital is growing. The 2024 and 2025 final rules added meaningful orthopedic and musculoskeletal procedures to that list. The infrastructure for physician-owned, high-quality, cost-effective surgical care exists. It is not theoretical.
What’s missing is physicians who are willing to take the risk to build it.
Indiana Orthopedic Institute is built around exactly this model: physician-owned, data-driven, patient-first care in an ASC environment. Our cost per episode is lower than comparable hospital-based care. Our patient satisfaction is not a talking point. It is a measured outcome that we track and publish. We didn’t do this because it was easy. We did it because the hospital model was not delivering what our patients deserved, and we knew how to build something better.
That is what the data on physician employment trends is really measuring. It is measuring the rate at which the profession is surrendering the ability to do what we did.

What the Next Decade Demands
The physicians who entered medicine in the last decade were trained during the consolidation era. For many of them, employment isn’t a compromise. It is the only model they’ve ever known. That is a problem, because you cannot fight for something you’ve never experienced.
In the South, the number of non-independent physicians increased by 106.7% over the eight-year period. Non-physician-owned practices grew by 140.2%. That is not a regional anomaly. That is a preview of what happens when consolidation runs unchecked.
Here is what I would tell every physician still early enough in their career to make a different choice:
Understand the contract before you sign it. Not the salary line. The non-compete radius. The termination clause. The productivity metrics that trigger consequences. The section that governs who owns the patient relationship if you leave. Read those sections three times, then have a lawyer read them again.
Study the ownership model before you dismiss it. The ASC path is not available to everyone in every geography. But more physicians could pursue it than do. The barrier is usually not regulatory or financial. It is psychological. The perceived safety of employment is hard to walk away from. But perceived safety and actual security are not the same thing.
Build something before you need to. The window is narrowing. Between 2024 and 2026 alone, nearly 24,000 more physicians shifted out of independent practice. Every year that passes, the market consolidates further, the referral networks lock tighter, and the cost of starting something independent increases.
Find physicians who are building. Not just complaining. Building. The complaint industry in medicine is enormous and entirely unproductive. What moves the needle is people constructing actual alternatives. Find those people. Learn from them. If you can, join them.
What I Know After 10,000 Surgeries
I trained at Mayo Clinic. I have an engineering degree. I have published research in top-tier journals. I sit on the boards of the largest orthopedic surgery organizations in the world. I have operated on more than 10,000 patients.
I am telling you that none of that insulates you from a system that will grind you into a production unit if you let it.
The 18% of physicians still practicing independently are not unicorns. They are not lucky. Most of them made a harder choice at a moment when the easier path was available. Some of them failed before they succeeded. A few of them built something that proved the model works.
That 18% number is not a ceiling. It does not have to keep falling. But it will, unless physicians who understand what is being lost decide that losing it is not acceptable.
The hospital systems are not going to save you. The professional organizations are not moving fast enough. The policy environment is improving in some areas and deteriorating in others.
The only durable answer is building the thing yourself.
That is what we did at Indiana Orthopedic Institute. It was hard. It was worth it.
The question is not whether the model works.
The question is whether you’re willing to build it.

This is a powerful observation, especially because it highlights a growing structural tension between clinical practice and administrative framing of care.
Once doctors are talked about like parts of the machine, it’s not hard to see why the work starts feeling less like medicine and more like output.