

The Physician Shortage Nobody Is Preventing
We know exactly how this ends. We're doing it anyway.

I had a conversation recently with a third-year surgical resident who told me she was seriously considering leaving medicine. Not because she didn’t love operating. Because she had spent the previous Friday doing 11 prior authorization requests instead of seeing patients.
She is 29 years old. She has $310,000 in medical school debt. She trained for seven years to use her hands and her judgment to help people. And the system handed her a fax machine and a denial queue.
We are burning our own pipeline. And the people in charge have every financial reason to keep doing it.
The Numbers Are Not Projections Anymore. They’re Arrivals.
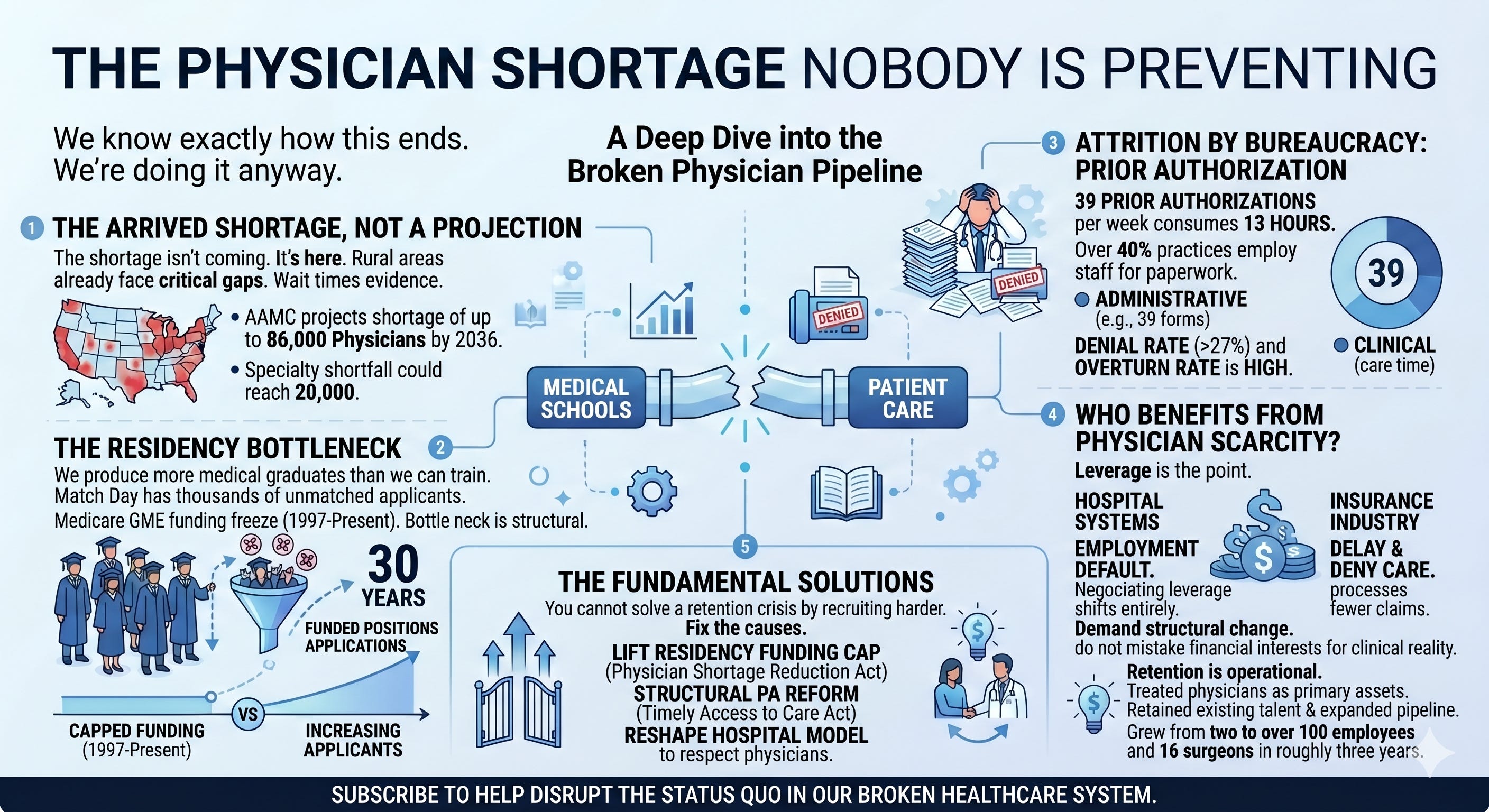
According to the Association of American Medical Colleges, the United States is on track for a shortage of up to 86,000 physicians by 2036. The surgical specialty shortfall alone could reach nearly 20,000. These are not speculative estimates from advocacy organizations with an agenda. This is the AAMC, the body that accredits medical schools and tracks physician supply nationwide, issuing a structural warning that has gone largely unaddressed for over a decade.
The shortage isn’t coming. It’s here. In rural counties, it arrived years ago. In specialty care, the wait times are already the evidence.
And while the supply side of the equation gets the headlines, almost nobody is talking honestly about what is destroying the supply we already have.
39 Prior Authorizations a Week. Every Week.
The American Medical Association surveys physicians every year on the prior authorization burden. The 2024 results: physicians complete an average of 39 prior authorization requests per week. That consumes roughly 13 hours of physician and staff time, every single week. More than 40% of physician practices now employ staff whose entire job is processing prior authorization paperwork.
Let me translate that into clinical time.
13 hours a week is nearly a full working day and a half. For a surgeon, that is two to three cases. For a primary care physician, that is 20 to 25 patient appointments. Vanished. Not into care. Into a bureaucratic process designed, explicitly, to slow down and deny access to treatments physicians have already determined are medically necessary.
Here is the number that should end the debate: more than 27% of physicians report that prior authorization requests are often or always denied. More than one in four requests, rejected outright. And when physicians appeal those denials, the overturn rate is extraordinarily high, which tells you exactly how valid the original denials were.
This is not a quality control mechanism. It is an attrition strategy. And it is working.
Who Benefits from a Doctor Shortage
I want to name something that rarely gets named directly: the physician shortage is not an accident, and it is not uniformly a problem for every player in the healthcare system.
Hospital systems benefit from it. When physicians are scarce and burned out, hospital employment becomes the default. The negotiating leverage shifts entirely. A physician with $300,000 in debt, no independent practice infrastructure, and a specialty that requires expensive equipment and facility access does not have many options. The hospital knows that. The employment contracts reflect that.
95% of physicians report that prior authorization somewhat or significantly increases physician burnout, according to the AMA. Burnout drives early retirement. Burnout drives physicians out of clinical practice and into administrative roles. Burnout drives that third-year resident to start reconsidering her career before she has even fully started it.
Every physician who exits the clinical workforce early is a physician who did not need to be recruited, trained, or competed for. The shortage creates leverage. The leverage is the point.
The insurance industry benefits from it too. A system with fewer physicians, longer wait times, and more administrative friction processes fewer claims. Prior authorization exists to delay and deny care. A burned-out physician who stops fighting denials, who stops appealing, who just moves to the next patient because there are 40 more in the queue, is an insurance company’s ideal outcome.
I am not describing a conspiracy. I am describing aligned financial incentives. In my experience, those are more dangerous than conspiracies because nobody has to coordinate them. The system just selects for behaviors that serve the system.
The Residency Bottleneck Nobody in Congress Will Fix
Here is the structural problem that sits underneath all of it.
The number of federally funded residency positions has been effectively capped since 1997, when the Balanced Budget Act froze Medicare Graduate Medical Education funding. Medical schools have expanded. Applications have grown. The physician pipeline has more people trying to enter it. But the bottleneck, at the residency level, has barely moved in nearly 30 years.
We are producing more medical school graduates than we can train. Match Day, the annual ritual where medical students learn whether they secured a residency position, has thousands of unmatched applicants every year. These are people who completed four years of medical school, passed licensing examinations, and cannot enter the workforce because there are not enough funded training slots.
The fix is not complicated. It requires Congress to lift the residency funding cap. The AAMC has recommended it. The AMA has recommended it. It has bipartisan support at the conceptual level. It has gone nowhere for a generation because the financial interests that benefit from physician scarcity are better organized than the patients who need more physicians.
That is the honest answer.

What We Did Instead
When I was building Indiana Orthopedic Institute, I made a specific decision early: we were going to create an environment where surgeons wanted to practice, not one where they felt trapped.
That meant eliminating the administrative noise that drives physicians out of medicine. It meant building ASC infrastructure that returns decision-making authority to the surgeon. It meant aligning financial incentives so that the people generating clinical value participate in the value they generate. And it meant treating physicians as the primary asset of the organization, not as a cost center to be managed.
We grew from two people to over 100 employees and 16 surgeons in roughly three years. I am not telling you that to impress you. I am telling you because the retention argument is operational, not theoretical. Physicians stay when the environment respects them. They leave when it doesn’t.
The national conversation about the physician shortage keeps returning to supply-side solutions: expand medical schools, extend scope of practice to non-physician providers, use AI to increase efficiency. Some of those have merit at the margins. But none of them address the fundamental mechanism driving physicians out of the profession they trained for.
You cannot solve a retention crisis by recruiting harder. You have to fix what is causing the exits.
What Has to Happen
The residency funding cap needs to be lifted. Full stop. The Physician Shortage Reduction Act has been introduced in multiple congressional sessions. It has not passed. Patients in underserved areas continue to wait.
Prior authorization needs structural reform, not voluntary pledges from insurance companies. The AMA has been advocating for the Improving Seniors’ Timely Access to Care Act for years. It addresses only Medicare Advantage. The broader problem remains untouched.
And hospital systems need to understand that the employment model they depend on is consuming the workforce they need. You cannot squeeze physicians indefinitely and expect the pipeline to keep filling.
To the residents and young physicians reading this: the system will tell you this is just how it works. That the prior authorizations, the administrative burden, the eroding compensation, the loss of clinical autonomy are the price of practicing medicine. That is not medicine. That is what happened to medicine. And it is not inevitable.
Build your own path if you can. Demand structural change if you can’t. And do not mistake the system’s financial interests for clinical reality.
The patients need you in the OR, not on the phone with a denial department.

Without addressing workflow inefficiencies and incentives, supply gains will continue to leak out of the system.