

The Stryker Cyber Attack That Just Proved My Point
And why it matters more than you think

Yesterday morning, a patient looked up at me from the pre-op table and asked why we weren’t using a robot for her knee replacement.
I told her exactly what I believe: “I do not want your surgery to be dependent on something that could get hacked, disrupted by a power outage, or derailed by a software glitch.”
She smiled and said, “Good. I didn’t want a robot doing my surgery anyway.”
By the time I finished her case, Stryker’s global network was down.
What Happened Today, And Why It Matters More Than You Think
A major cyberattack crippled Stryker’s global networks today, with an Iran-linked hacking group claiming responsibility and calling it “the beginning of a new chapter in cyber warfare.”
The group, Handala, claims to have wiped more than 200,000 servers, mobile devices, and other systems, forcing Stryker to shut down offices in 79 countries.
They also claim to have extracted 50 terabytes of data, which they are threatening to make public.
As of tonight, Stryker is still investigating the breach and does not know when its systems will be back online. In a regulatory filing Wednesday afternoon, the company acknowledged it expects disruptions to continue and that “the timeline for a full restoration is not yet known.”
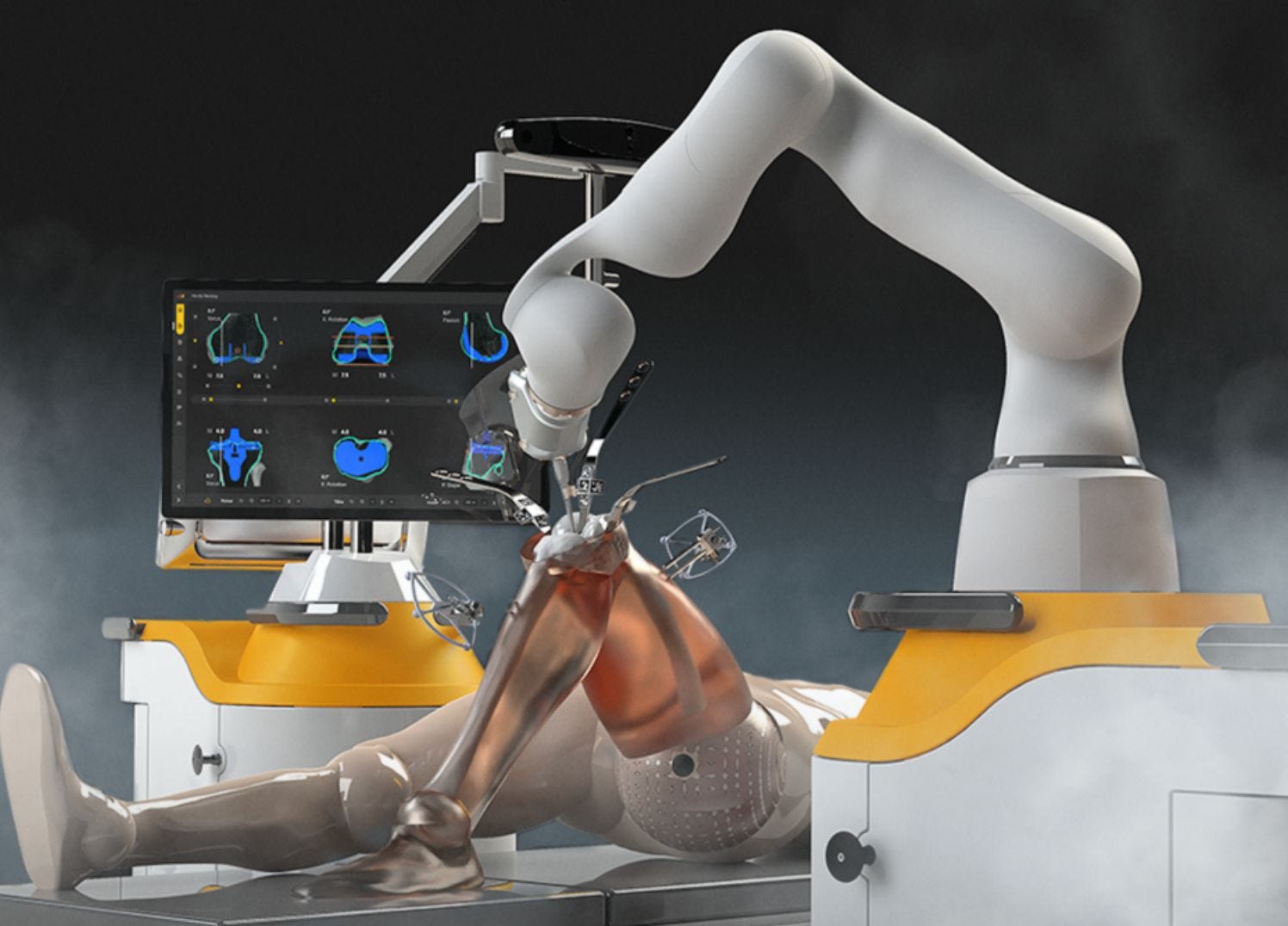
Stryker. The company behind Mako. The number one robotic surgery platform in orthopedics. Offline. Globally. Today.
I have written about the over-reliance on robotics in orthopedic surgery before. I have said in boardrooms, in lecture halls, and in published research that the obsession with robotic dependency is creating risk, not eliminating it.
I want to be precise today, because precision matters: this is not about Stryker being a bad company. I have respect for many of their engineers and clinical teams. This is about something far more dangerous than any single company’s security posture.
This is about what happens when we build a healthcare system that cannot function without a network connection.
I Am One of the Few People Positioned to Say This Clearly
As an engineer, researcher, entrepreneur, inventor and surgeon with decades of experience… I am not just a commentator on this topic. I am a practitioner who has been inside the operating room, inside the boardroom, and inside the regulatory and research infrastructure that governs how these technologies are adopted, promoted, and too often, blindly accepted.
When I say robotics has a rightful place and a dangerous misapplication, I am speaking from 20 years of lived evidence. Not a whitepaper. Not a conference panel. The OR.
The Vulnerability We Built Ourselves
Here is the uncomfortable truth that nobody in the robotics-industrial complex wants to say out loud:
Over-utilization and over-dependency on any single technology creates systemic fragility, and in surgery, fragility kills.
Stryker produces equipment used in hospitals and surgical settings across orthopedics and neurosurgery, and reports its products reach more than 150 million patients annually across 61 countries. That scale is extraordinary. It is also exactly what makes a single point of failure catastrophic.
When a geopolitical conflict (US-Iran tensions, in this case) can reach into a Michigan headquarters and wipe 200,000 devices overnight, we have to ask a harder question than “how do we fix Stryker’s cybersecurity?”
We have to ask: What happens to the patients when the robot can’t connect?
I designed my practice around a principle that the engineering community has known for decades: redundancy and human override are not optional features. They are the architecture. The surgeon is not the backup plan. The surgeon is the plan. Technology augments that. Technology does not replace it.
When we flip that hierarchy, when the robot is the plan and the surgeon is the override, we have not improved care. We have introduced a catastrophic dependency.
The Status Quo Indictment
For the last decade, hospital systems and device companies have sold robotics as the future of surgery. The pitch is seductive: sub-millimeter precision, reproducibility, reduced variability. And there is real science behind some of those claims. I do not dispute that robotics, used correctly, adds value.
But “used correctly” is doing enormous work in that sentence.
What I have watched instead is a market-driven race to robotic adoption that has outpaced the clinical evidence, inflated hospital capital expenditure, and begun to erode the one thing that cannot be hacked, disrupted, or wiped: the trained human mind operating at the point of care.
Cybersecurity experts told CNN on Wednesday they were on alert following the attack, with one expert noting that Russia, about a decade ago, created a “global malware epidemic” when it released malware on a small target that wasn’t confined.
The lesson is not new. Interconnected systems have interconnected vulnerabilities. We have simply chosen not to apply that lesson to surgical infrastructure.
I will apply it now: every time we make a surgical outcome dependent on a networked system, we have introduced a new attack surface into the doctor-patient relationship.
That is not hyperbole. That is engineering.
A Personal Moment of Reckoning
I have had my own confrontations with this question, not in the abstract, but in the OR.
Early in the life of Indiana Orthopedic Institute, I had a case where a technology I trusted performed outside its expected parameters. The outcome was ultimately fine.
But in that moment, standing at the table, I was reminded of something that no device company will ever put in a brochure: the surgeon is the last line of defense. Not the software. Not the implant. Not the algorithm.
Me. My training. My hands. My judgment built over 10,000 cases.
That moment recalibrated something for me. Technology earns trust incrementally, in my OR, through demonstrated outcomes, not through marketing claims, hospital purchasing agreements, or robot utilization bonuses embedded in surgeon compensation packages.
The day I let a system tell me what the right answer is, without my own clinical override, is the day I stop being a surgeon and start being a technician.
The Blueprint: Technology in Its Rightful Place
This is not an anti-technology argument. I want to be precise about that, because it will be misread. I use technology every day. Indiana Orthopedic Institute is built on data, innovation, and research. We are actively engaged in developing the next generation of surgical tools.
But there is a framework I operate by, and today’s attack makes it more urgent than ever.
The Surgeon-First Technology Hierarchy:
The surgeon makes the clinical decision. Technology informs that decision. It does not override it.
Every networked dependency is a risk variable. It must be evaluated as such, not marketed around.
The patient relationship is local, analog, and human. It cannot be outsourced to a cloud.
Redundancy is not a fallback. It is the standard of care.
Technology that cannot function without a network connection has no place as the primary driver of a surgical outcome.
At Indiana Orthopedic Institute, we built around these principles from day one, not because we were anti-technology, but because we are engineers who understand systems. A system that fails catastrophically under a single point of attack is a poorly designed system. Full stop.
What This Means for Every Surgeon Reading This
The hospital systems that pushed robot utilization metrics on you will not call you today to apologize for the dependency they built.
The device companies that incentivized robotic adoption through volume agreements and capital placement deals will issue a press release about their cybersecurity response and move on.
The insurance-industrial complex will file this under “operational disruption” and wait to see if premiums need adjusting.
You are the one standing at the bedside. You are the one your patient trusted this morning when she asked whether you were going to use the robot, and when you told her no, she exhaled.
That exhale is data.
The geopolitical reality we are living in, where a pro-Iran hacking group can cause a global network disruption at one of the largest medical device companies in the world as an act of retaliation for military strikes, is not going away.
If anything, the attack surface is growing. Every networked surgical dependency we add is a new vulnerability we hand to adversaries we cannot control.
The answer is not to stop innovating. The answer is to stop confusing innovation with dependency.
Build your clinical autonomy now. It is not a luxury. Today proved it is a survival skill.

A system that can operate safely, even when technology fails, protects patients first.
Spot on. This why one needs to have what I call a human centric approach and not just a human in the loop approach.