

They Told Me to Cool It. I'm Not Going To.
Followup to my article and podcast about the Stryker Cyber Attack

I woke up Thursday morning to a text message from a colleague.
“You need to cool it on LinkedIn. You’re making yourself look bad.”
That was jarring for about 30 seconds. Then I thought about the patient I saw Wednesday morning, the one who said she was glad I don’t use a robot. I thought about the Stryker attack that hit the same day.
And I thought about the 10x more messages I received privately from surgeons and healthcare leaders who said: keep going, we need this conversation.
So no. I’m not cooling it.
Let Me Be Precise About What I Actually Said
The pushback I received on LinkedIn was, in a word, telling.
Robotic surgeons came out saying their robots were working fine. Nobody was harmed. Quit fear-mongering.
With respect: that was not my point. And the fact that so many people misread it tells me exactly how threatened they felt.
I am not anti-robot. I have been using computer navigation since 2011, over a decade before many of these same surgeons adopted any intraoperative technology. I am an engineer. I co-design devices. I sit on the boards that govern the future of orthopedic innovation. I am one of the few people in the world with real standing on both sides of this table.
My point was simple: a cyberattack on the largest producer of robotic surgical technology is a wake-up call. If we are not honest about what that means for patient safety, we are failing the people who trusted us with their lives.
That is the thing I will not apologize for.
The Dots Are Connecting. Is Anyone Watching?
Three things are happening simultaneously in orthopedics right now, and almost no one is connecting them out loud.
First, surgical robotics has moved toward automated function, where control is being removed from the surgeon’s hands. The largest implant company in the world recently acquired a fully autonomous robot. That is not incremental. That is a fundamental shift in where accountability lives.
Second, the industry is migrating to cloud-based, interconnected ecosystems because the data doesn’t have much value sitting in isolation on the robot. Everyone is moving it to shared servers and remote data centers.
Third, healthcare represents 20% of US GDP. If a country we are in active conflict with wants to destabilize us, where do they aim?
Stryker industry representatives in Indiana woke up Wednesday with blank phones. Wiped. Across 79 countries.
Autonomous robots plus cloud connectivity plus healthcare as a geopolitical target equals an attack surface we have handed to our adversaries ourselves. I don’t hear anyone at the robotics meetings I attend talking about cybersecurity. Not once. And I’m in those rooms.
We need to start talking about it.
The Data Nobody Wants to Cite
Let me be precise here, because in my first article I understated the numbers. The Australian registry data is worse than I initially quoted.
The study examined robotic-assisted partial knee replacement using the Mako system and found that revision for infection was 2.91 times more likely compared to non-robotic implants over the entire study period, and 5.57 times more likely in the critical zero-to-three month window immediately after surgery. That early window is when surgical site infection, the kind most directly linked to what happened in the operating room, does its damage.
Three to five and a half times more likely to have a postoperative infection. That is not a rounding error. That is a signal.
Again, registry data establishes correlation, not causation. My clinical theory is that longer operative times and the added complexity of managing a large mechanical device in a sterile field are contributing factors. The data on operative time and infection risk is very strong and well established. But whatever the mechanism, that correlation exists in the peer-reviewed literature, and it deserves honest scrutiny, not silence.
If robotic and navigation-guided manual surgery produce equivalent outcomes, you still have to answer a harder question: why are we adding significant cost and potentially elevated infection risk to a healthcare system already at its breaking point?
I told Dennis Berry on the podcast: I would rather take that extra money and give it to a pediatric leukemia patient. The deployment of healthcare dollars has to be proportional to impact. That is not politics. That is math.
What the Actual Adoption Numbers Show
I quoted roughly 25% robotic penetration in knees on the podcast. The 2025 American Joint Replacement Registry data tells a more nuanced story, and it is worth looking at carefully.
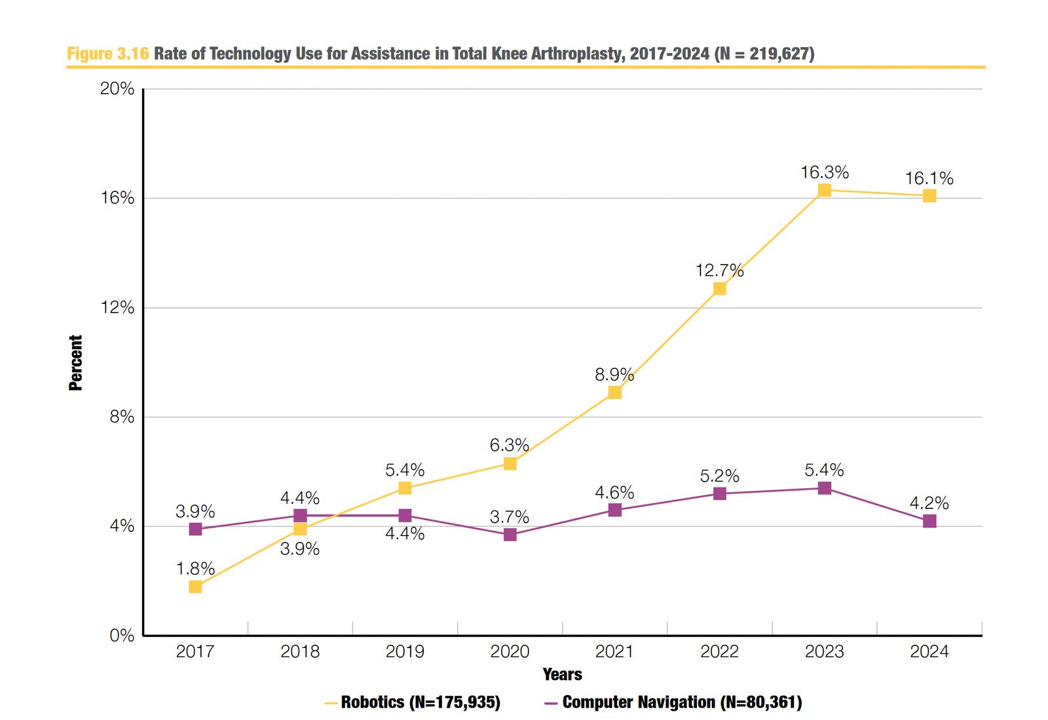
[Figure 3.16 - Rate of Technology Use for Assistance in Total Knee Arthroplasty, 2017-2024] Robotics grew rapidly from 1.8% in 2017 to a peak of 16.3% in 2023, then actually declined to 16.1% in 2024. Computer navigation has remained essentially flat the entire period, hovering between 3.7% and 5.4%.
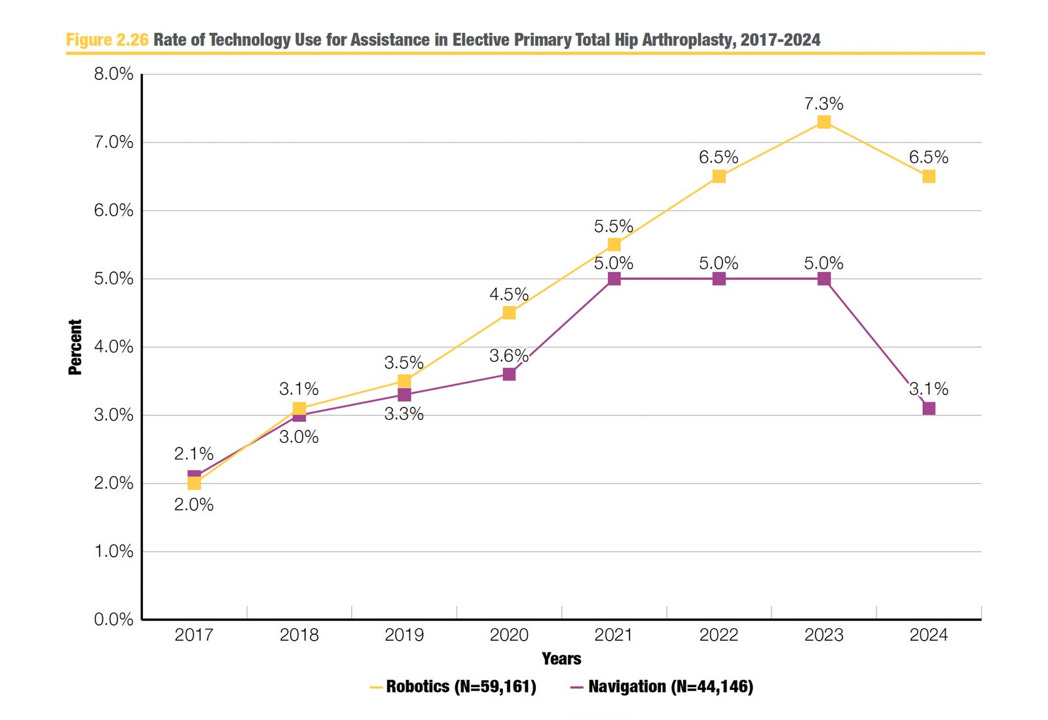
[Figure 2.26 - Rate of Technology Use for Assistance in Elective Primary Total Hip Arthroplasty, 2017-2024] Robotics in hip replacement peaked at 7.3% in 2023 and declined to 6.5% in 2024. Navigation similarly dropped from 5.0% to 3.1% in the same year.
Read that again. Robotic adoption in both hip and knee replacement declined from 2023 to 2024.
I will be the first to say that one year of decline does not establish a trend. But combined with the infection data from Australia, and with what I am hearing from residents and fellows on the ground, it is at minimum a data point worth taking seriously. Something that is truly transforming a field does not plateau and decline at 16% in knees and 6.5% in hips.
That is the data. Not my opinion. The data.
The Training Gap Nobody Is Admitting
This is the one that keeps me up at night.
Orthopedic surgery residents applying to our fellowship at Indiana Orthopedic Institute have started specifically seeking programs without heavy robotics training. I asked why. They said: because I haven’t done many surgeries without it. And I’m scared.
We have already heard of surgeries canceled because the robot was down and the surgeon lacked the confidence to operate without it. We have heard of a robot failing mid-case and the surgeon unable to complete the procedure. I didn’t even want to know the rest of that story, but I heard enough.
I use the airline industry as a frame. The gray-haired pilots flying 350 people across the Atlantic have built manual skill that no autopilot dependency ever erased. When Sully Sullenberger landed on the Hudson River, no algorithm saved those passengers. Forty years of training, judgment, and human hands did.
Surgeons are the pilots of the operating room. We are building a generation who may only know how to fly with autopilot on.
I am sounding that alarm now.
The Liability Question Coming Faster Than You Think
Two months ago, a colleague at a major East Coast academic center told me they had just hosted a lecture on medical liability and AI. The emerging legal consensus: the companies producing AI will bear liability for AI-driven clinical decisions.
Some physicians hear that and exhale. Not my problem anymore.
Think carefully about what comes next. The moment you surrender your accountability to an algorithm, you surrender your authority. And the moment you surrender your authority, you will be paid like a technician, not a surgeon.
We are the ones cutting human beings open. That ethical weight does not transfer to a server.
What the Balance Actually Looks Like
This is not anti-technology. This is not anti-robot. This is not anti-innovation.
This is a demand for appropriate deployment, proportional investment in protection, and honest conversation about risk.
If you are going to connect patient-level technology, literally inside someone’s body, to a cloud-based ecosystem, invest 10 times as much in cybersecurity as you do in the technology itself. That will slow things down a little. Good. Not all innovation is perfect innovation. When a car is going out of control, you check the brakes.
No patients were harmed in the Stryker attack. This was a warning shot, a stress test, a rare moment where the system revealed its vulnerability before someone paid for it on the table. We should be grateful. And we should act like it.
Keep the surgeon, the trained human being with decades of judgment in their hands, as the primary driver of every surgical decision. That is patient-first care. That is the oath.
I am in Milan next week working on the next worldwide knee system we are launching at Indiana Orthopedic Institute. Innovation is very much alive here. We just refuse to build it on a foundation of dependency and denial.
The conversation is not over. It is just getting started.
Dr. Michael Meneghini
Founder and CEO, Indiana Orthopedic Institute & The Incision Point
Watch the full podcast with Dennis Berry on the Elite Leaders Substack.

And if you disagree, say so here. I’ll be in the comments.
Great follow up article. The open, honest discussion you bring to the table with the willingness to actually discuss and not just angrily argue is a breath of fresh air!
Speaking up matters, especially when patient safety, cybersecurity, and the future of surgical care are at stake.